Open Chest Tube Clearance of Clot: Is it safe? Is there a better way?
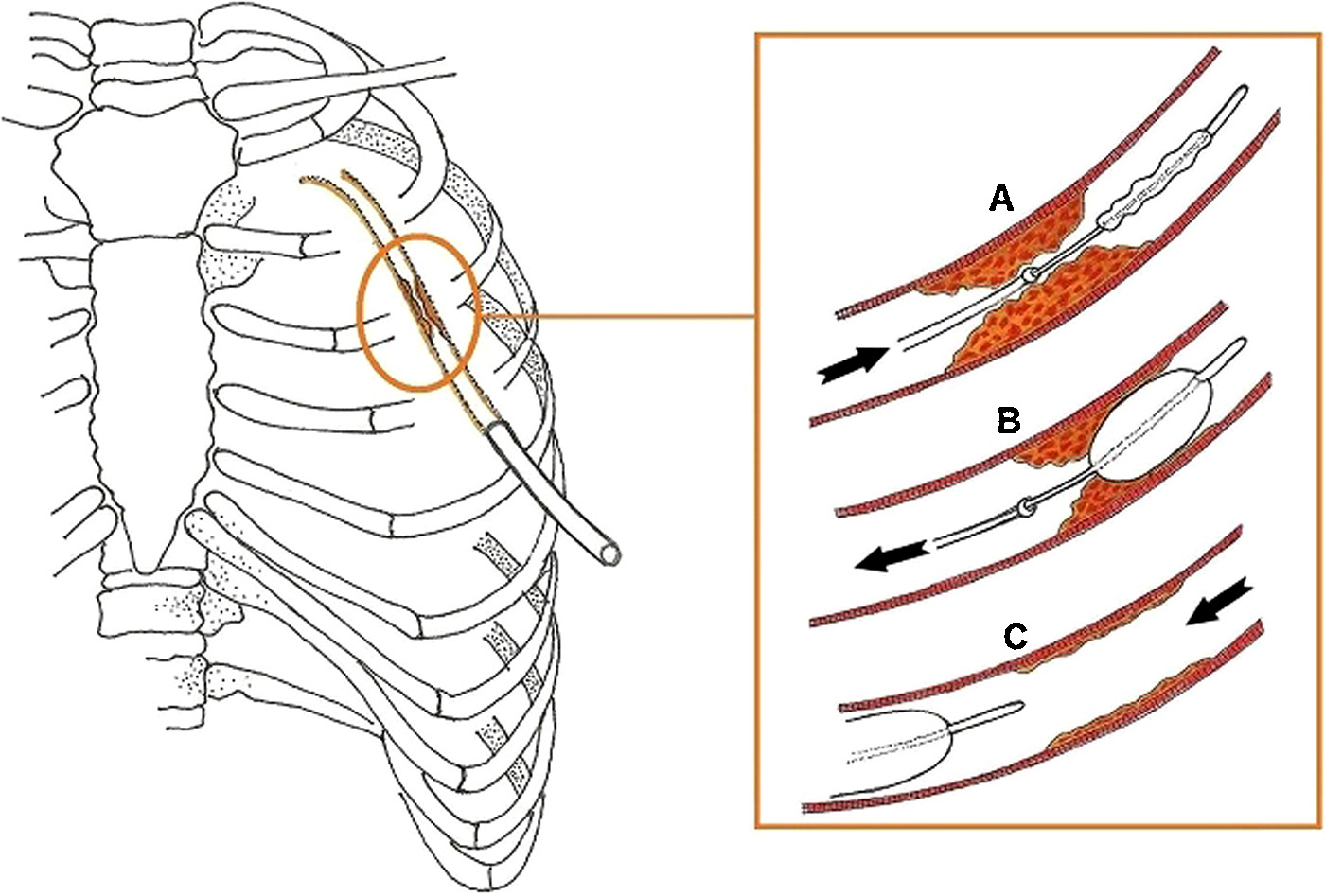 Image from Ref. 1, Boyacioglu et al.
Image from Ref. 1, Boyacioglu et al.
Chest tubes are required for all heart operations to evacuate shed blood from around the heart and lungs. Evidence suggests that nearly 36% of chest tubes can clog, preventing adequate blood evacuation and potentially leading to retained blood syndrome (RBS).
But how do you keep chest tubes free of clot and working to evacuate shed blood? There are currently no published national standards, and thus nurses and ICU care givers are left to make bedside, makeshift efforts to address this common problem on their own.
In addition to the questionable techniques of milking and stripping, one such bailout technique is open clearance of the chest tube once it is noticed that tube stops working. In this case, the caregiver stops what they are doing, sets up a “sterile field” by putting down a sterile towel, touches up the connection from the drainage tube to the chest tube with an antiseptic, then opens the chest tube so they can advance either a suction catheter or Fogarty balloon catheter into the chest tube to clear it of clot. 1, 2
This approach raises a lot of questions:
- Is this really a safe procedure at the bedside in the ICU?
- Can this lead to infection since one has to break the sterile seal?
- How far do you blindly push in the catheter? Can you injure an organ internally if it goes out the tip or a side hole?
- Does this even work? Might it be too late to make a difference?
- How often is this done?
- Who should do this?
- Is this cost effective?
- Is the Fogarty Balloon or suction catheter regulatory approved for that purpose?
There are no great answers to these questions, which is one reason perhaps its use should be limited. This is a standard “bailout” technique, trying to react to a problem after it’s noticed, rather than prevent a problem before it happens. There are obvious drawbacks and pitfalls.
Perhaps there is a better way. PleuraFlow Active Clearance Technology allows one to proactively clear chest tubes without breaking the sterile field. In a recently published paper in the Journal of Thoracic and Cardiovascular Surgery, Retained Blood syndrome was reduced by 43%. This has the advantage of allowing ICUs to have proactive chest tube clearance protocols with a regulatory approved product, rather than leaving the team to react with potentially harmful makeshift, off label bedside methods such as open suction or balloon catheter clearance of chest tubes. Is it time your program consider Pleuraflow?
1 Boyacioglu K, Kalender M, Ozkaynak B, Mert B, Kayalar N, Erentu? V. A new use of Fogarty catheter: chest tube clearance. Heart Lung Circ. 2014;23:e229Ye230.
2 Halejian BA, Badach MJ, Trilles F. Maintaining chest tube patency. Surg Gynecol Obstet. 1988;167:521.